A Medical Device Maker's Guide to FDA Cybersecurity Testing for 510(k) & PMA
Contributors


The rules of engagement need to reflect pharma-specific constraints that a generic pen test provider may not anticipate. No active testing on production validated systems without an approved test environment. No testing during batch manufacturing runs. Change control documentation for any activity that touches a validated system, even in a test environment. These constraints do not limit what the test can find. They ensure that what the test finds is actually actionable.
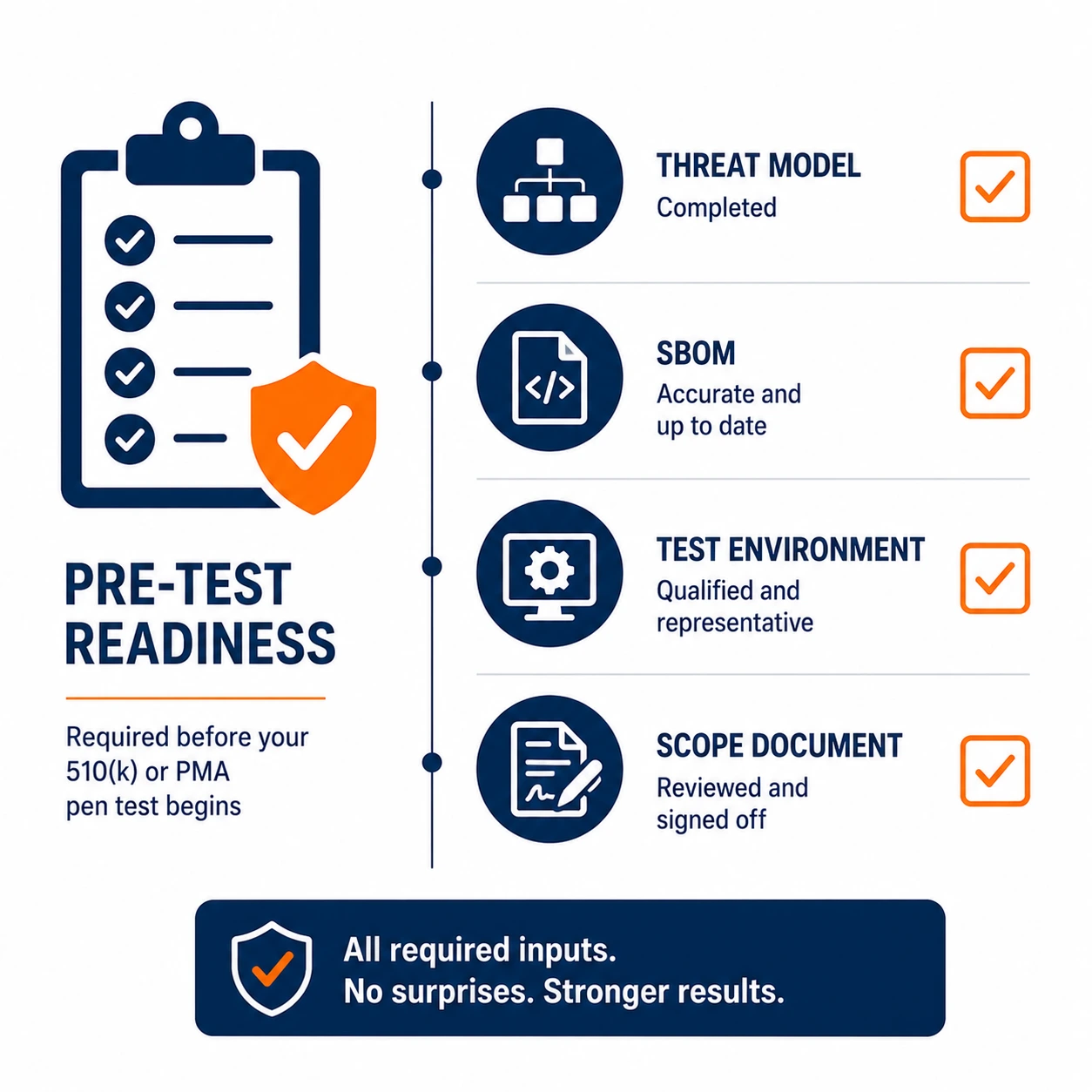
Before the Test: What Must Be in Place
A pen test submitted as FDA cybersecurity evidence is only as credible as the foundation it was built on. FDA reviewers evaluate pen test evidence in the context of the threat model and SBOM that should precede it. A test conducted without a documented threat model looks like a box-checking exercise. A test conducted without a complete SBOM raises questions about whether the tester knew what they were testing.
The threat model must reflect the device's intended use environment and the realistic threat actors relevant to that environment. A patient monitor deployed in an ICU connected to a hospital network faces threats from opportunistic attackers exploiting hospital network access, from insiders with legitimate network presence and from targeted actors interested in patient data or care disruption. The pen test methodology should be calibrated to those threats, not to a generic enterprise IT threat model.
During the Test: What Must Be Covered
FDA guidance identifies specific categories of testing that cybersecurity submissions should address. Hardware interface testing covers physical ports, debug interfaces and any physical access mechanism that could be exploited. A USB port that accepts unsigned firmware updates is a finding. An exposed JTAG interface with no access controls is a finding. These are not theoretical vulnerabilities; they are the kind of hardware-level weaknesses that have appeared in real device compromises.
Software and firmware testing covers known vulnerability validation, authentication mechanisms and update integrity. Can a malicious firmware update be installed without cryptographic verification? Can the device be accessed without valid credentials through an undocumented interface? Does the device's software contain components with known vulnerabilities that have not been patched? Each of these questions needs a documented answer in the submission.
Communication Interface Testing
For most connected devices, communication interface testing is where the most significant findings emerge. Wireless protocol testing covers Bluetooth pairing security, Wi-Fi authentication and any proprietary wireless protocol the device uses. TLS implementation testing validates that encrypted communications are actually secure: certificate validation is enforced, weak cipher suites are not accepted and the device cannot be subjected to downgrade attacks.
The FDA pays particular attention to how devices authenticate to backend systems and how they handle communication with mobile applications. A device that accepts connections from any app presenting the right device identifier without additional authentication creates patient safety risk that reviewers are trained to identify.
After the Test: What the Evidence Package Must Contain
The pen test report submitted to FDA needs to contain more than a standard commercial findings report. It needs to document the scope in terms that map to the device's SSP and threat model. It needs to map each finding to the relevant design control and risk management file entry. It needs to document the remediation status of every finding, including those that remain open with an accepted risk justification.
Unresolved findings are not automatically disqualifying, but they require documented justification. A finding that was assessed, determined to be acceptable given the intended use environment and mitigating controls, and documented as an accepted risk with a compensating control is a defensible position. A finding that appears in the report with no remediation status or justification is not.
The Patch Management Plan
Section 524B requires a postmarket patch management plan as part of the premarket submission. FDA reviewers look for evidence that the manufacturer has a realistic, tested process for monitoring vulnerabilities, assessing their relevance to specific device models and deploying patches in a timeframe proportionate to risk severity. A policy document that describes what the process will be is not the same as evidence that the process works.
Pen testing has a role in validating the patch management process as well as in the initial submission. Testing that a critical vulnerability fix actually closes the vulnerability, rather than just checking a box, is the kind of postmarket validation the FDA expects manufacturers to demonstrate capability for.
Frequently Asked Questions
The FDA does not publish a single checklist, but its guidance, Section 524B, and reviewer expectations point to three testing categories a submission should address: hardware interface testing, software and firmware testing, and communication interface testing. Each category needs documented answers to specific questions, and the whole test must be grounded in a threat model and software bill of materials that were established before testing began.
Two foundations must exist before testing: a documented threat model and a complete software bill of materials. FDA reviewers evaluate pen test evidence in the context of both. A test run without a documented threat model reads as a box-checking exercise, and a test run without a complete SBOM raises the question of whether the tester actually knew what they were testing. The credibility of the evidence depends on this foundation.
The threat model must reflect the device's intended use environment and the realistic threat actors for that environment, not a generic enterprise IT model. A patient monitor in an ICU connected to a hospital network faces opportunistic attackers exploiting hospital network access, insiders with legitimate network presence, and targeted actors interested in patient data or care disruption. The pen test methodology should be calibrated to those specific threats.
Hardware interface testing covers physical ports, debug interfaces, and any physical access mechanism that could be exploited. A USB port that accepts unsigned firmware updates is a finding. An exposed JTAG interface with no access controls is a finding. These are not theoretical weaknesses: they are the kind of hardware-level flaws that have appeared in real device compromises, which is why FDA reviewers expect them to be tested and documented.
Software and firmware testing covers known vulnerability validation, authentication mechanisms, and update integrity, and each area maps to a specific question the submission must answer. Can a malicious firmware update be installed without cryptographic verification? Can the device be accessed without valid credentials through an undocumented interface? Does the device's software contain components with known, unpatched vulnerabilities? Each question needs a documented answer in the submission.
Because most connected medical devices depend heavily on their communication paths, and those paths carry the highest-impact weaknesses. Communication interface testing covers wireless protocol security, such as Bluetooth pairing and Wi-Fi authentication, and TLS implementation, verifying that certificate validation is enforced, weak cipher suites are rejected, and the device resists downgrade attacks. For many devices, this is the category that surfaces the findings reviewers care about most.
The FDA pays particular attention to how a device authenticates to backend systems and how it communicates with mobile applications. A device that accepts connections from any app presenting the correct device identifier, with no additional authentication, creates a patient safety risk that reviewers are specifically trained to identify. Testing must demonstrate that these connections are properly authenticated, not just functional.
The report needs more than a standard commercial findings list. It must document the scope in terms that map to the device's system security plan and threat model, map each finding to the relevant design control and risk management file entry, and document the remediation status of every finding, including any that remain open. This mapping is what lets a reviewer connect the testing to the device's overall safety and risk documentation.
No. Unresolved findings are not automatically disqualifying, but they require documented justification. A finding that was assessed, determined acceptable given the intended use environment and mitigating controls, and documented as an accepted risk with a compensating control is a defensible position. A finding that appears in the report with no remediation status or justification is not, and that gap is what creates a problem in review.
Section 524B requires a postmarket patch management plan as part of the premarket submission, and reviewers look for evidence that the process actually works, not just a policy describing what it will be. Pen testing validates the process by confirming that a critical vulnerability fix truly closes the vulnerability rather than just checking a box. That kind of validation is the postmarket capability the FDA expects manufacturers to demonstrate.



Other Popular Articles
In the digital age, businesses must adopt an ad
GRC is the capability, or integrated collection
Get the latest insights straight from our desk to your inbox.
Other Featured Articles
Explore More
What Is CMMC and Do You Need It?
Learn what CMMC is, who needs it, and how to determine if your business requires Level 1 compliance for DoD contracts.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
CMMC Level 1 vs Level 2, Which Applies to You?
Learn the key differences between CMMC Level 1 and Level 2, understand FCI vs. CUI, and determine which CMMC level your DoD contract requires to avoid unnecessary costs or compliance risks.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
What CMMC Means for DoD Subcontractors
Understand what CMMC means for DoD subcontractors, how compliance requirements flow down from prime contractors, who must comply, and the steps to determine your CMMC obligations.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
How to Complete Your CMMC Level 1 Self Assessment
Complete CMMC Level 1 self-assessment guide: define scope, work through 15 practices, fix common gaps, and submit your SPRS affirmation.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
The October 2026 CMMC Deadline: What Happens If You Miss It
Prepare for the October 2026 CMMC deadline. Learn how compliance affects DoD contract eligibility, SPRS affirmations, renewals, and subcontractors.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Operational Technology (OT) Penetration Testing Guide for Ransomware Defense
Ransomware doesn't need to breach your control room it needs to get close enough that you can't trust it hasn't.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
A Medical Device Maker's Guide to FDA Cybersecurity Testing for 510(k) & PMA
The FDA doesn't publish a pen testing checklist, but its guidance, 524B requirements, and reviewer expectations add up to one.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Pharma Pen Testing: Why FDA and IP Risk Need Different Scoping
Standard pen test scoping frameworks weren't built for pharma.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
FDA 524B Is Here: What Medical Device Makers Must Test Now
Section 524B made medical device cybersecurity a legal requirement, not a guideline.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Why CHIPS Act Manufacturers Can't Rely on CMMC Pen Testing Alone
Semiconductor manufacturers face dual compliance obligations under CMMC 2.0 and the CHIPS Act and a standard pen test satisfies neither fully.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Why Pen Test Evidence Fails C3PAO Assessments (and How to Fix It)
Completing a pen test isn't enough for CMMC.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
PTaaS vs. Annual Pen Testing: Why Manufacturers Are Switching
Annual penetration testing produces documentation, not security.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Map Your OT Attack Surface Before the Next Audit
Don't wait for an auditor to tell you what you missed.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
How to Scope IT-OT Penetration Testing Safely
Learn how to safely scope IT-OT penetration testing engagements.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
How Often Should Manufacturers Run OT Penetration Testing?
Annual pen testing fits a budget cycle but it doesn't reflect how fast manufacturing environments actually change.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Pharmaceutical Pen Testing: What 21 CFR Part 11 and cGMP Require
21 CFR Part 11 and cGMP don't mention penetration testing but the controls they require depend on it.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Pharmaceutical Pen Testing: Why R&D and GxP Need Different Scopes
R&D and GxP regulated environments have different risk profiles, compliance requirements, and testing constraints.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Why Pharmaceutical Pen Testing Must Address Nation-State Threats
Nation-state actors treat pharma like critical infrastructure targeting formulation data, synthesis routes, and clinical IP with patience and precision.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
How Ransomware Crosses the IT-OT Boundary (And How to Stop It)
Ransomware operators target the IT-OT boundary deliberately and they know manufacturing economics well.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
Where Industry 4.0 Left Your OT Attack Surface Wide Open
Industry 4.0 connected OT environments were never built for. Learn why traditional IT security tools fall short and what OT penetration testing reveals that audits miss.
Shantanoo Govilkar
SVP Strategic Solutions Risk & Cybersecurity Solutions view
What AS4 Actually Solves: Real Outcomes Companies See After Migration
Discover what AS4 actually solves for modern businesses. Learn the real outcomes companies achieve after migration, from stronger security to better B2B integration performance.
EDI Solutions Group
Marketing Group view
7 Migration Pitfalls That Derail AS4 Upgrades (and How to Avoid Them)
Avoid costly AS4 upgrade mistakes. Discover 7 migration pitfalls that delay projects, create risk, and disrupt B2B messaging, plus practical ways to avoid them.
EDI Solutions Group
Marketing Group view
How to Perform Penetration Testing in Cloud Environments (AWS, Azure, and GCP) - 2026 Edition
A practical guide to cloud penetration testing across AWS, Azure, and GCP. Learn methods, tools, and best practices to identify vulnerabilities and improve security.
Cybersecurity Solutions Group
Marketing Group view
5 Signs It's Time to Move Legacy EDI Environment to AS4 Protocol
Partner onboarding delays, compliance gaps, and rising maintenance costs are signals your EDI infrastructure is reaching its limits. Learn the five signs it is time to evaluate a move to AS4.
EDI Solutions Group
Marketing Group view
How to Design Custom Chatbots That Cannot “Make Stuff Up”
Confident AI answers without traceable sources create institutional risk. Learn how Grounded RAG architecture retrieves real documents first and attaches verifiable citations to every response.
Data and AI Solutions Group
Marketing Group view
How Citation-Backed Conversational AI Improves Public Access and Internal Decision-Making
AI without source citations creates real liability. Learn how citation-backed AI brings traceable sources, version awareness, and audit-ready outputs to every institutional decision.
Data and AI Solutions Group
Marketing Group view
How to Perform a Successful Network Penetration Test: Comprehensive Guide for 2025
Learn how to perform a successful network penetration test to identify vulnerabilities, simulate real cyberattacks, and strengthen your organization’s network security.
Cybersecurity Solutions Group
Marketing Group view
What Is Penetration Testing? A 2026 Expert Guide
A 2026 expert guide to penetration testing for security leaders and IT teams seeking proactive defense, compliance, and stakeholder trust.
Cybersecurity Solutions Group
Marketing Group view
OT Ransomware Prevention: Practical Best Practices for Industrial Cybersecurity
Explore enterprise grade OT ransomware prevention strategies, including segmentation, identity control, threat informed detection, and resilient recovery design to protect industrial operations fro
Cybersecurity Solutions Group
Marketing Group view
10 Myths About OT/ICS Security That Put Your Business at Risk
Think your OT network is secure? Learn the 10 most dangerous myths about OT and ICS cybersecurity that leave industrial operations exposed to attacks.
Cybersecurity Solutions Group
Marketing Group view
OT Ransomware Risks and Response for Industrial Systems
Learn why OT environments face higher ransomware risk, how attackers gain access, and how effective detection and response reduce operational impact.
Cybersecurity Solutions Group
Marketing Group view
AI Risk Assessment: Risk Types, Best Practices & More
Explore AI risk types, essential assessment frameworks, and proven best practices to mitigate threats in AI deployment. Learn actionable strategies for secure AI systems today.
Cybersecurity Solutions Group
Marketing Group view
AI Risk Assessment: Everything You Need to Know
Learn essential processes, methodologies, risk types, regulatory requirements, and practical implementation strategies for safe AI deployment.
Cybersecurity Solutions Group
Marketing Group view
Whitepaper: Ransomware Threat Management
Ransomware continues to be a real threat to business operations across all industries, no organization is safe from this threat.
Laszlo S. Gonc
CISSP, First Senior Fellow, DivIHN Cybersecurity Center of Excellence view
Cybersecurity Incident Response Preparedness
An incident response framework provides a structure to support incident response operations. A framework typically provides guidance on what needs to be done, but not on how it is done.
Laszlo S. Gonc
CISSP, First Senior Fellow, DivIHN Cybersecurity Center of Excellence view
IoT Medical Device Cybersecurity
Healthcare data and medical devices would be aggressively targeted by ransomware attacks since early 2017 has proven to be true